


Written by: Hart Edmonson, MD (NUEM ‘27) Edited by: David Adler, MD (NUEM ‘25)
Expert Commentary by: Anthony J. Esposito, MD
Expert Commentary
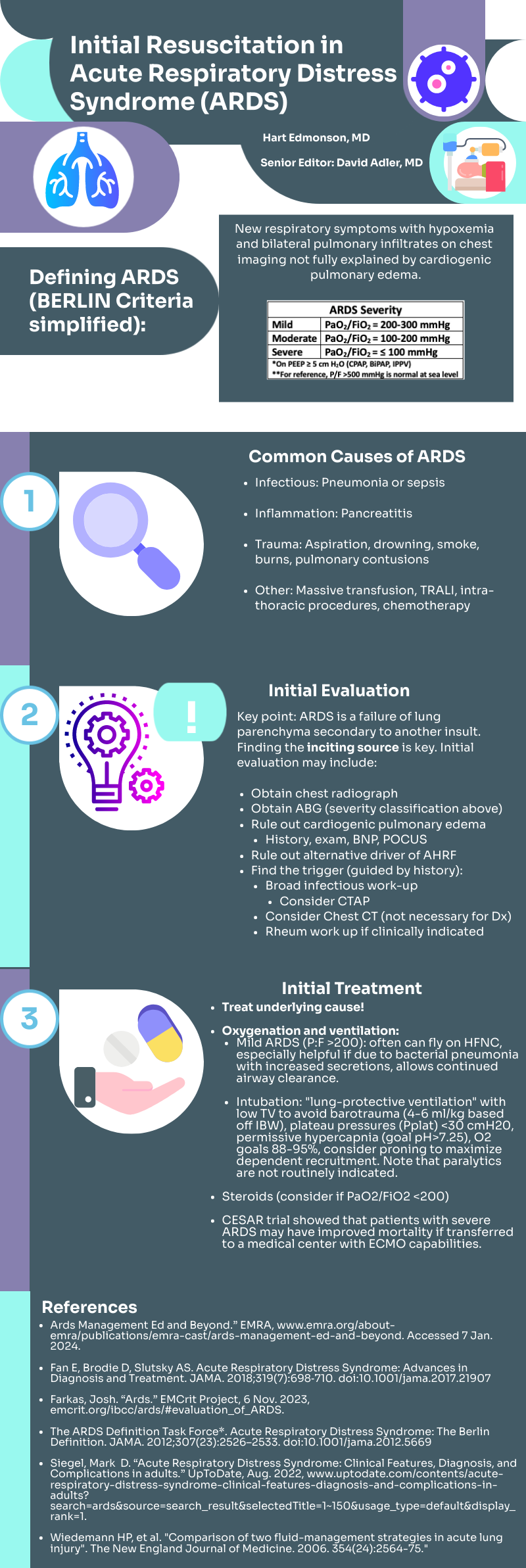
Thank you to Drs. Edmonson and Adler for this infographic that concisely emphasizes key concepts for the recognition and initial management of acute respiratory distress syndrome (ARDS) in the Emergency Department. ARDS should be considered in patients with progressive dyspnea and hypoxemia and with bilateral alveolar infiltrates on chest imaging who have been exposed to an “inciting source” within one week (and often hours) of presentation. Contrary to the recency bias of many, ARDS is not just a phenomenon associated with COVID-19. Indeed, there are many inciting sources that can be divided into direct—pneumonia, aspiration, intrathoracic procedures—and indirect—non-pulmonary sepsis, pancreatitis, trauma/burns, blood product transfusion (“TRALI”)—lung injury. As the clinical presentation of ARDS is nonspecific, a high degree of clinical suspicion is necessary to initiate timely supportive measures in the Emergency Department and to mitigate the high degree of associated morbidity and mortality. Chest imaging and an arterial blood gas are essential to establishing the diagnosis and severity of disease. While cardiogenic pulmonary edema can coexist and is difficult to distinguish acutely, it cannot be the sole cause of the observed imaging abnormalities.
There is no cure for ARDS, and the cornerstone of care is early initiation of supportive measures. Guidelines strongly emphasize the use of “lung protective ventilation” (outlined in this infographic) in addition to early consideration of prone ventilation (>12 hrs/day), the latter specifically for patients with P:F < 150. Corticosteroids are increasingly being recognized as an adjunct early in care for patients with ARDS while late administration (>2 wks after onset) may increase risk of death. High PEEP with continuous monitoring of respiratory mechanics and hemodynamics can support oxygenation while neuromuscular blockade can be considered for significant ventilator dyssynchrony. Careful selection of refractory cases for VV-ECMO is advised (P:F < 80 or refractory respiratory acidosis with pH < 7.25).

Anthony J. Esposito, MD
Assistant Professor, Medicine (Pulmonary and Critical Care)
Northwestern Memorial Hospital
How To Cite This Post:
[Peer-Reviewed, Web Publication] Edmonson, H. Adler, D. (2024, Jul 15). Initial Resuscitation in ARDS [NUEM Blog. Expert Commentary by Esposito, AJ. Retrieved from http://www.nuemblog.com/blog/initial-resus-in-ARDS









