

Author: Erik Handberg, MD (EM Resident Physician, PGY-2, NUEM) // Edited by: Greg Apel, MD (EM Resident Physician, PGY-4, NUEM) // Expert Reviewer: Kelly Williamson, MD
Citation: [Peer-Reviewed, Web Publication] Handberg E, Apel G (2016, March 29). Myocarditis In The ED. [NUEM Blog. Expert Peer Review by Williamson K]. Retrieved from http://www.nuemblog.com/blog/myocarditis-in-the-ed/
The Patient
An otherwise healthy 38-year old male presents with 2 days of retrosternal chest tightness after recent recovery from a upper respiratory infection. He notes that his upper respiratory symptoms have resolved but he continues to experience excessive fatigue, low grade fever and body aches. The patient appears in mild respiratory distress with audible bibasilar crackles at his lung bases.
An EKG is obtained which demonstrates significant sinus tachycardia. Cardiac biomarkers return with severe elevation in troponin I concerning for acute ischemia. Cardiology is consulted. In order to help distinguish between ACS and myocarditis a focused bedside echo is performed:
Apical 4-chamber view demonstrating moderate-to-severely depressed LVEF with global hypokinesis without pericardial effusion.
Myocarditis
The scenario above is concerning for the development of acute myocarditis. Myocarditis is an inflammatory change of the heart muscle and an important differential diagnosis for patients presenting with non-specific symptoms such as low grade fever, fatigue, malaise, dyspnea on exertion, palpitations, and/or chest pain (most commonly sharp, pleuritic and positional but can also be squeezing and retrosternal). In the absence of significant chest pain these vague symptom often lead physicians to miss the diagnosis on initial presentation. Although 40-50% of patients will report antecedent viral illness, multiple other etiologies have been described including non-viral infectious, drug-related, autoimmune, and post-partum myocarditis.
Etiologies
Medical Decision Making & Work Up
The vague symptoms these patients present with make this a difficult to diagnose condition in the emergency room and a high clinical suspicion must be maintained. As a emergency physician, initial consideration should also be focused on other life threatening presentations of chest pain and dyspnea (Box 3).
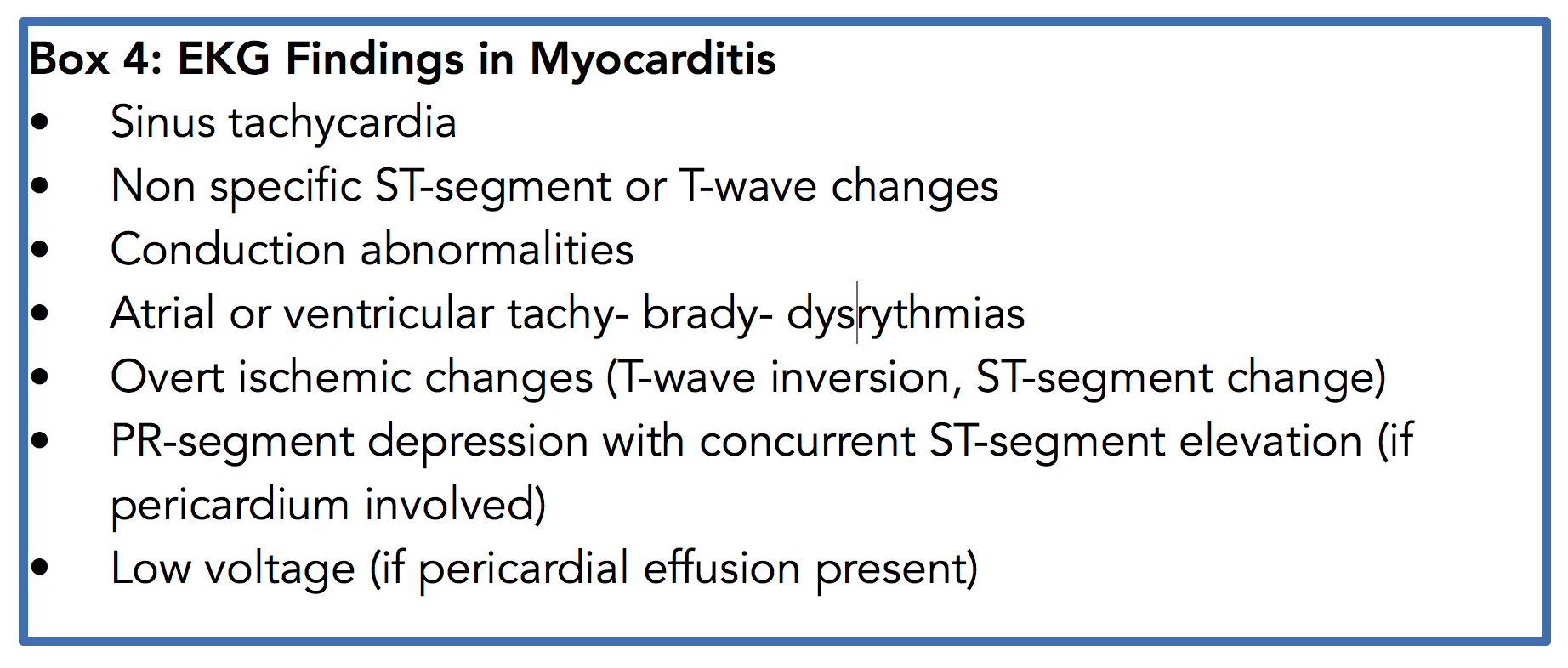
The EKG will be abnormal the majority of the time, but is often non-specific (Box 4). Focal myocarditis may mimic acute myocardial infarction with clear ischemic evidence on ECG. On physical exam, features of heart failure may be present including: jugular venous distention, bibasilar crackles, audible third heart sound and lower extremity swelling.


Work up in the emergency room should include standard chest pain evaluation with EKG, cardiac biomarkers, blood count, chemistry and chest x-ray. Further imaging and labs should be dictated by your active differential diagnosis. Cardiac biomarkers will sometimes be elevated in myocarditis. In this case, focus should be directed on ruling out ischemia first. Serial cardiac biomarkers are helpful as levels do not tend to rise and fall as quickly with myocarditis as with myocardial infarction. Echocardiography (Box 5) may be useful as adjuvant imaging in the emergency department, especially when attempting to differentiate between ACS and myocarditis.
Treatment
Generally, the emergency room treatment of myocarditis is directed at subsequent effects of cardiac damage caused by inflammation and subsequent myocardial destruction. Focus should be maintained on the ABCs of resuscitation. Signs of congestive heart failure and hypoxia should be treated with oxygen, preload/afterload reduction, and diuresis. Treat any dysrhythmias if they are present. Sympathomimetic and beta-blocker therapies have been shown to worsen myocardial necrosis and worsen mortality, and should be avoided. Immunosuppressive therapies are of unproven benefit unless the patient has known immune mediated disease. NSAIDs are contraindicated in early and acute-phase myocarditis due to increased myocardial damage. If the patient presents in shock, maintain perfusion through use of vasopressors (norepinephrine) and inotropic agents (dobutamine). Critical care, cardiology and infectious disease should be consulted early in patients with signs of severe heart failure as more advanced therapies such as ventricular assist devices and intraaortic balloon pumps may be required.
Take Home Points
- Consider myocarditis in patients with non specific symptoms (i.e low grade fever, fatigue, malaise, dyspnea on exertion, etc) and an abnormal ECG
- Keep your differential diagnosis open if myocarditis is suspected and rule out other life threatening causes of chest pain and dyspnea
- Bedside echocardiography can be accurately used to grossly assess left ventricular function as well as rule out a pericardial effusion which can be present in up to 25% of myocarditis cases. It may also assist in differentiating between myocarditis and ischemia though this should be done in collaboration with cardiology.
- Treatment for myocarditis should focus first on ABCs of resuscitation as well as management of heart failure symptoms and dysrhythmias. Avoid sympathomimetics, beta blockers and NSAIDs.
- Critical care, cardiology and infectious disease consultation should be considered early, along with formal echocardiography, and admission to appropriate level of care depending on clinical status.
Expert Review
Dear Dr. Handberg,
Thank you for presenting an excellent review on the topic of myocarditis; emergency physicians must maintain a high index of suspicion for this disease process in the appropriate clinical setting as it can be difficult to diagnose yet rapidly fatal. While relatively uncommon, especially compared with other causes of chest pain such as acute coronary syndrome, complications of myocarditis are presumed to cause 20% of cases of sudden death in young adults and it is a leading cause of dilated cardiomyopathy worldwide. In the pediatric population, undiagnosed myocarditis is one of the common diagnoses involved in emergency department malpractice claims.
As you astutely noted, the primary key to diagnosis of fulminant myocarditis is the development of rapidly progressive decompensated heart failure in a previously healthy patient. However, the clinical spectrum of myocarditis varies from those patients who are relatively asymptomatic to those who rapidly develop heart failure and fatal arrhythmias and the diagnosis for those patients presenting with more subtle symptoms remains the most challenging. In the case of viral myocarditis, obtaining a history of antecedent illness is helpful and the diagnosis must at least be considered in patients presenting with fever and chest pain or those with persistent unexplained tachycardia. As myocardial biopsy is the gold standard for diagnosis, we must look for alternate useful tests in the emergency department. Lab testing, while not sensitive or specific for the diagnosis, may be helpful when examined in the appropriate clinical context. For instance, troponin elevation raises concern for myonecrosis and higher levels of troponin have been shown to have prognostic implications [1]. In addition, nonspecific biomarkers of inflammation including CRP and ESR can be elevated in myocarditis, though a normal value does not exclude the disease process. As noted in box 4, EKG findings are equally nonspecific, though findings such as persistent sinus tachycardia and T wave inversions, especially in a previously healthy individual, are concerning. In the case of myopericarditis, the more classic diffuse saddle-shaped ST segment elevation with PR depression can be present. Interestingly, certain EKG findings are related to long-term cardiac outcome: QTc prolongation >440ms, abnormal QRS axis, and ectopic ventricular beats are associated with a poor clinical outcome and a QRS duration >120ms was found to be an independent predictor for death or heart transplant [2]. As a result of these determinations, the EKG is more useful as an easily accessible tool for risk stratification than as one that confirms diagnosis.
In terms of more advanced imaging, there are no specific echocardiographic features of myocarditis, though can be utilized to exclude other causes of heart failure such as valvular disease and, as noted in box 3, provide information as to the global function of the heart. While it may not be readily available in the ED setting, cardiovascular MRI can be a useful diagnostic study as the technology can detect changes in the myocardial tissue as early as the first stage of inflammation.
The mainstay of treatment for myocarditis involves addressing the heart failure with pharmacologic agents such as diuretics, nitroglycerin, and ACE inhibitors. In addition to the agents that you discussed, milrinone can augment cardiac function in those patients presenting with decompensated symptoms. Alternative therapies that have been explored include systemic corticosteroids, which have demonstrated beneficial effects in small case series and randomized control trials [3], though this data is confounded by the fact that the majority of adults recover spontaneously without intervention. Finally, a Cochrane review from 2015 found no evidence to suggest that use of intravenous immunoglobulin (IVIG) is beneficial in adults [4]. For those patients with refractory symptoms despite optimal medical management, one may ultimately consider LVAD, temporary ECMO, and heart transplant.

Kelly Williamson, MD
Assistant Residency Program Director Advocate Christ Medical Center; Clinical Assistant Professor at UIC
References
- Lauer B, Niederau C, Kuhl U. Cardiac troponin T in patients with clinically suspected myocarditis. J Am Coll Cardiol. 1997 Nov 1; 30(5): 1354-1359.
- Ukena C, Mahfoud F, Kindermann I, Kandolf R, Kindermann M. Bohm M. Prognostic electrocardiograhic parameters in patients with suspected myocarditis. Eur J Heart Fail. 2011 April; 13(4): 398-405.
- Aziz, KU; Patel, N; Sadullah, T; Tasneem, H; Thawerani, H; Talpur, S (October 2010). "Acute viral myocarditis: role of immunosuppression: a prospective randomised study". Cardiology in the young 20 (5): 509–15.
- Robinson, J; Hartling, L; Vandermeer, B; Klassen, TP (20 May 2015). "Intravenous immunoglobulin for presumed viral myocarditis in children and adults.". The Cochrane database of systematic reviews 5: CD004370.
- Cosby KS, Kendall JL. Practical Guide to Emergency Ultrasound. Lippincott Williams & Wilkins, Philadelphia. 2006.
- Moore CL, Rose GA, Tayal VS, Sullivan DM, Arrowood JA, Kline JA. Determination of left ventricular function by emergency physician echocardiography of hypotensive patients. Acad Emerg Med.2002;9:186-193.
- ACEP Echocardiography for Emergency Physicians. http://www.sonoguide.com/cardiac.html#cardref5
- Rosen & Barkin’s 5-Minute Emergency Medicine Consult. Wolters Kluwer Health. Philadelphia. 5th edition. 2015.
- Ledford DK: Immunologic aspects of cardiovascular disease. JAMA 1992; 268: pp. 2923
- Brady WJ, Ferguson JD, Ullman EA, et al: Myocarditis: emergency department recognition and management. Emerg Med Clin North Am 2004; 22: pp. 865
- Felker G, Boehmer J, Hruban R, et al. Echocardiographic findings in fulminant and acute myocarditis. J Am Coll Cardiol. 2000;36(1):227-232. doi:10.1016/S0735-1097(00)00690-2.
- Kindermann I et al. Update on Myocarditis. J Am Coll Cardiol. 2012; 59(9): 779-792.
- Ong P et al. Usefulness of pericardial effusion as new diagnostic criterion for noninvasive detection of myocarditis. Am J Cardiol. 2011; 108(3): 445-52.
- Magnani J et al. Myocarditis: Current Trends in Diagnosis and Treatment. Circulation. 2006; 113: 876-890.
- Adams, J Emergency Medicine Philadelphia, PA: Saunders, 2008. Print